
Hospitals mandating flu vaccines
If vaccines are safe, the United States wouldn't have the Vaccine Injury Compensation Trust Fund—but it does.
I went from being an influenza vaccine advocate to one who thinks that its avid proponents are either poorly informed (as I once was) or insufficiently intelligent to connect the dots.
This article provides an eye-opening look at this issue in addition to exposing how unscrupulous people put their desire for money ahead of your health concerns. I also reveal the danger of hospital executives with more power than brains. Even if you never step foot in a hospital, their mistakes could kill you or a loved one.
The effectiveness of influenza vaccines is often exaggerated and the usefulness of other preventive measures is typically ignored, which is odd: if disease prevention is the goal, why not present the complete story? Why? Because the focus of the medical profession is more to sell drugs and profit from administering them than fostering health—something most doctors are woefully ignorant of. I could prove that by showing how little most MDs know about health, but you can prove it to yourself just by looking at doctors, many of whom are overweight and not very healthy or happy.
Take me, for example. I graduated in the top 1% of my class in medical school (therefore, I stayed awake in it) but I was an overly cynical and bitter sourpuss after working as an ER doc wore me down UNTIL I discovered a natural and healthy secret not taught in med school or residency that's basically the missing link to happiness and feeling good—like having an internal smile that lasts all day long.
While I am in good shape and look (and act) young for my age, almost none of the knowledge enabling that came from medical school; I read about health beginning at age 14, and I still do that, up to three hours per day now and 16 hours daily in the past. Most other doctors are not that devoted to health … and it shows!
After reading the evidence cited below, you might conclude that I oppose influenza vaccines. No, I advocate putting them into perspective and yearly evaluating their risks and benefits, then choosing the best vaccine available (they are NOT identical; example) and administering it in the best possible way, but at no time do I fall for the flu vaccine hype that gives too many people a false sense of security.
- Influenza vaccines are not nearly as effective as their supporters claim. Their efficacy and safety are given an undeserved luster by research in which medical whores are paid to distort the truth.
- Hospitals that purport to care about patients carelessly endanger them in many other ways.
- How hospitals feed on patients like vultures—and how to fight back.
Is that all? No. You will also learn how a vitamin offers better protection from influenza and other infectious diseases, why nurses are paid less than they deserve, why nonprofit hospitals are hell-bent on profiting from you, how drug reps use sex to sell drugs, what really paralyzed Franklin D. Roosevelt (hint: not polio), why some hospital awards are as meaningful to me as those in Cracker Jack® boxes, how hotshot CEOs are often just the beneficiaries of luck—not talent, how hospitals bend over backwards to give better care to VIPs, why more doctors don't speak up, why hospitals don't solve even solvable problems, how we could remedy our most pressing national economic problems, and why smear merchants will lie through their teeth about people who want to help others so their bosses can stay in power to help themselves. The common denominator in these seemingly diverse topics is the key to comprehending why the flu vaccine hype is just a sliver of a much bigger problem.
UPDATE 5/17/2016: Differences in individuals' immune responses linked to flu vaccine effectiveness
Natural compound coupled with specific gut microbes may prevent severe flu
A high-fiber diet protects mice against the flu virus
To truly understand this issue, you must know what flu vaccine supporters don't know or wish you didn't know. I'm going to spill the beans on some of the dirty little secrets of the healthcare industry, which has made a mint by keeping you in the dark. I'll figuratively turn on the lights so you can see what those rats have been up to.
Once you connect the dots, you will be mad as hell if you're not blind as a bat in seeing what will soon be obvious to intelligent people: that the influenza vaccine distortions are just a microcosm of what's wrong in the world today. Want to find out? Grab a cup of coffee, put your feet up, and continue reading.
UPDATE May 16, 2013: A few years after I published this article, Dr. Peter Doshi, a researcher at the prestigious Johns Hopkins University School of Medicine, connected the dots and is questioning U.S. public health agency advice on influenza vaccines, just as I have.
He said two influenza vaccine studies the CDC cites to support its case are “simply implausible” and likely result from the healthy-user effect, adding that “there is virtually no evidence that influenza vaccines reduce elderly deaths.”
In an article published in the prestigious BMJ, Dr. Doshi wrote that the “enormous growth [in influenza vaccine use in the U.S.] has not been fueled by popular demand but instead by a public health campaign that delivers a straightforward, who-in-their-right-mind-could-possibly-disagree message: influenza is a serious disease, we are all at risk of complications from influenza, the flu shot is virtually risk free, and vaccination saves lives.”
But the flu vaccine reality doesn't match the hype. Our leaders, who should have known better, and most doctors—who too readily accept the snake-oil messages from drug companies—have overstated the benefits and understated the risks of influenza vaccines. Dr. Doshi is clearly disgusted by this disregard for the truth, saying “Closer examination of influenza vaccine policies shows that although proponents employ the rhetoric of science, the studies underlying the policy are often of low quality, and do not substantiate officials’ claims. The vaccine might be less beneficial and less safe than has been claimed, and the threat of influenza appears overstated.”
Based on what Dr. Doshi wrote about Nancy Snyderman, MD (the chief medical editor for NBC News), she appears to need a summer school lesson in logic. But as I suggested in an article about the über-gorgeous Dr. Jennifer Ashton, TV docs are often selected on the basis of appearance, not brainpower. Dr. Ashton is hardly a dumbbell, but there are smarter and more knowledgeable physicians—so why not hear from them instead?
Health is a life-and-death matter. I'd prefer first-rate information from docs with second-rate appearance instead of second-rate information and analysis from docs with first-rate appearance. I bet you would, too. But the mainstream media that is so adept in being cheerleaders for Big Government is sucking up to other teats, including Big Pharma and Big Food.
Most journalists can't differentiate fact from fiction, as if their brains have been numbed by an overdose of system justification. Whatever their masters want them to believe, they swallow hook, line, and sinker, proudly passing along propaganda like good little mindless robots happy to do the dirty work for masters who can't rule the world and profit from it without distorting the truth and pulling the wool over the eyes of sheeple trained to not think for themselves.
Excerpt from Pharmaceuticals: A Market for Producing 'Lemons' and Serious Harm, Analysis Finds: “The pharmaceutical industry is a "market for lemons," a market in which the seller knows much more than the buyer about the product and can profit from selling products less effective and less safe than consumers are led to believe … ”
References:
- Influenza: marketing vaccine by marketing disease
- MIT grad shows CDC mind-behavior control duping doctors and public to buy vaccine
- Publication Of Flu Vaccines Studies In Prestigious Journals Are Determined By The Sponsor
- Medscape: It Ain't Necessarily So: Why Much of the Medical Literature Is Wrong
- From the Geisel School of Medicine at Dartmouth: Corruption of health care delivery system?
Excerpt: “The foundation of evidence-based research has eroded, experts say, and the trend must be reversed so patients and clinicians can make wise shared decisions about their health. Authors of a new report highlight five major problems set against a backdrop of 'obvious corruption.'” - If you think highly of drug companies, read this excerpt from FDA to Investigate Bayer's Essure Contraceptive Device: “[The FDA] has opened an investigation of the Essure (Bayer Healthcare Pharmaceuticals Inc) permanent contraceptive device after allegations that the company falsified and altered medical records during clinical trials, failed to report adverse events, deceived the public and the FDA about the device's safety and efficacy, and used defective materials in manufacturing, according to a petition from the Law Offices of Koch Parafinczuk & Wolf, PA.” (emphasis added)
No decrease in influenza after vaccination
Most reasonable people would agree that mandating an unproven drug is un-American if not downright unethical. However, that is exactly what it happening now as the approaching fall signals the beginning of the season to scare the bejesus out of people regarding influenza. Each year, the scare tactics ratchet up a notch or two. Recently, we've been led to believe that not getting the flu vaccine is akin to playing Russian roulette. The effectiveness of those histrionics is wearing thin as people enter winter after being given dreadful prognostications of the death toll, which never reaches the level of Black Death carnage predicted by the scaremongers.
Unproven? Says who? Says its manufacturer:
They admitted that “there have been no controlled trials adequately demonstrating a decrease in influenza disease after vaccination with FLULAVAL.”

In spite of that, many hospitals are now mandating influenza (flu) vaccines for their employees and medical staff. The ostensible reason for this demand is to protect patients. That seems reasonable, but it is specious and a glaring example of how hospital big shots are often bereft of common sense and blithely dismissive of patient and worker concerns and welfare.
If hospitals have the legal right to compel staff to receive the flu vaccine, why don't they have the legal right (and obligation to patients) to require vaccines for other infectious diseases, such as pneumococcal pneumonia and meningitis? They can be even deadlier than influenza. Before they become too ill to work, staff with those diseases can transmit germs to patients, just as they can with influenza. If the justification is because flu is more common, precisely what is the threshold of prevalence that gives hospital brass the legal right to tell workers what to do with their bodies? Is that codified somewhere, or is it just an improvised expedient concocted by people who think “because I said so” is sufficient grounds to threaten noncompliant workers with the loss of their jobs or, for doctors, loss of their medical staff privileges?

If prevalence is the excuse, why are hospitals so cavalier about staff sore throats, colds, and other common, easily transmitted infections? They are nothing to sneeze at because their mortality rate isn't zero. A previously healthy thirtyish friend who was not immunocompromised contracted a cold from one of her children, who recovered uneventfully, but she died from a complication. All of the many hospitals I worked in permitted obviously ill employees to work, many of whom felt pressure to do that, fearing that too many sick days would cost them their jobs.
No one needs a Petri dish and microscope to know that hospitals are teeming with potential sources of germs that can imperil patients, yet the geniuses who mandate flu vaccines usually turn a blind eye to these threats. I've seen countless blood pressure cuffs and EKG leads spattered with blood that stays on until it flakes or rubs off because, in my experience, those things were never cleaned.
Nurse and doctor uniforms “are usually colonized with potentially pathogenic bacteria, including drug-resistant organisms” such as Clostridium difficile and methicillin-resistant Staphylococcus aureus (MRSA), a primarily hospital-acquired superbug that kills more Americans than AIDS. Despite that risk, “some medical personnel wear the same unlaundered uniforms to work day after day.” Hospital computers, phones, pens, and stethoscopes can also harbor deadly germs. These threats endanger patients, but most hospitals do little or nothing about it but feel entitled to pat themselves on the back after yapping about the flu vaccine. It's trendy to overemphasize it while underemphasizing other preventable infectious diseases that deserve to share the limelight.
Simple tests to determine if your hospital is serious about preventing infections:
(1) Do all employees wear masks all of the time? Influenza is not the only serious illness!
(2) Do all employees wash their hands before and after patient contact, or at least change gloves with every patient contact?
(3) Do all employees properly don gloves? When applying typical (nonsterile) gloves instead of sterile ones for surgery, what almost invariably happens is that workers assume cleanliness doesn't matter because the gloves aren't sterile, so they fish them out of their box using “dirty” or improperly washed hands, thereby contaminating not only the outside of their gloves but other ones. With typically 100 to 200 gloves per box, plenty of hands contaminated from 1001+ sources transmit germs onto gloves, any one of which may be contaminated by dozens of workers. Then those gloves touch noses, eyes, genitals, or go into a mouth, rectum, or vagina. Or a phlebotomist may use them to draw blood, potentially spreading germs into a vein, hence into the blood and throughout the body. No restaurant serves sterile food, yet it obviously matters if your food is contaminated by unclean hands or gloves even though stomach acid is remarkably effective in killing many germs.
(4) Do all employees KNOW HOW TO PROPERLY wash their hands? A study showed that few (5%) people wash hands correctly. This meshes with what I've observed in hospitals. After I told one technician what she was doing wrong, she was unable or unwilling to do it correctly!
(5) Can ill employees call in sick without fear of reprisal, or are they pressured to work? Articles: Survey findings: 4 in 10 healthcare professionals work while sick and Working with influenza-like illness: Presenteeism among US health care personnel during the 2014-2015 influenza season. WHY employees do that is answered by my local hospital that penalizes people for calling in sick too often. I've been sick once in the past several (five? six? seven? it's so long I can't recall) years, but I know many tips to minimize disease transmission not known by most healthcare practitioners. When hospitals don't educate their staff with this info, they should not penalize them for suffering as a result. BTW, this is one of 1001 examples illustrating how hospitals don't know nearly enough about health to help themselves, let alone patients. American “healthcare” is less focused on health than on money and control.
(6) Do all employees know the many tips I know for preventing infectious disease transmission?
(7) If it mandates influenza vaccines, does it administer the best one? Giving cheaper trivalent vaccines instead of quadrivalent is a clear sign of perfunctorily fulfilling requirements instead of selecting the most effective one. But not all quadrivalent vaccines have equal efficacy: for example, a study “compared Flublok Quadrivalent to a licensed quadrivalent influenza vaccine made in eggs during the 2014/15 influenza season. The data showed that Flublok recipients were 43% less likely to develop culture confirmed influenza than people who received the traditional vaccine.” (See How flu shot manufacturing forces influenza to mutate based on A structural explanation for the low effectiveness of the seasonal influenza H3N2 vaccine and Faulty Flu Shots? Blame Eggs: Experts: growing virus in the humble breakfast staple hampers efficacy) I analyzed the data and chose Flublok Quadrivalent for my 2017 vaccine. Every hospital could do the same, but many prioritize second-rate care for employees so they can give first-rate pay to top leaders.
(8) If administered, where are vaccines given? Relevant research: Location, location, location: Immunization delivery site matters: cDC2 dendritic cells key to vaccine effectiveness. Excerpt: “ … the usual method, intramuscular injection, is likely not the most effective way to target those dendritic cells.”
I've worked in many hospitals, including prestigious university-affiliated ones in which most of their doctors and leaders thought they were Gods, yet not one came close to meeting ANY of the above criteria.
No hospital does as much as it could or should to minimize the risk of germ transmission. Too many of them look to easy, quick fixes such as the influenza vaccine that delude them into thinking they're doing enough to protect patients. Nonsense. They can't have workers change their uniforms more often? They can't clean their stethoscopes after each use? Too much work? Is it just too bad if a nosocomially acquired infection causes “flesh-eating” necrotizing fasciitis? It is difficult to put a price on patients losing precious parts of their bodies or going to their graves decades too early, but I'd like to think that whatever it costs to give healthcare workers the extra time they need to take such steps is well worth it.

want so much money?
Excerpt: “August 14, 2018 - Over the past decade, salaries for hospital CEOs have risen much faster than for surgeons, physicians, and nurses …”
October 19, 2023: Nonprofit hospitals skimp on charity while CEOs reap millions, report finds: Nonprofit hospitals got $28 billion in tax breaks—which made up 44% of their net income.
Moneygrubbing hospital executives may be a greater threat to patient safety than influenza. Their lavish pay, which often makes doctors seem like paupers, takes money away from workers—money that could be used to fund infection control measures.
Hospital leaders invariably boast of their concern for patients, but here is an acid test to determine if that is genuine or just hot air: Are they willing to donate all of their salary above $200,000 per year? That could be well over one million dollars that could pay for uniform changes, stethoscope disinfection, and other infection control measures that will unquestionably prevent serious diseases and even deaths. A hospital CEO would need rocks in his head to think those problems are less important than all the toys he could buy with the extra money.

$200,000 per year is enough to live a very good lifestyle, but many hospital big shots feel entitled to drain far more from the hospital coffers so they can own a private airplane, yacht, vacation home in Vail (Colorado), and home as large as a castle—perhaps necessary to house their immense egos. The small minds in their big heads deem such frivolity more important than disease and death in patients they profess to care so much about. What a farce!
Hospitals are often led by greedy hypocrites who think their avaricious desires are paramount, and patients are somewhere down the list. Few hospital leaders are worth what they are paid. They often rose to the top not by brilliance, but by a combination of Machiavellian scheming, reliance on the old boys' club, mutual back-scratching, the Peter Principle, and plain old luck.
I never made $200,000 per year as an ER doctor, but I offered to work for half-pay so my boss could afford to have me work twice as many hours. I did not like how ER patients often had to wait too long to be given too-rushed treatment, so I put my money where my mouth is and did something about it. How many hospital big shots will do the same?
Why hospital bills are outrageously high, and how to slash them
I was shocked by the staggering difference between what ER doctors are paid and what ER (or other hospital) patients are charged. Even if nurses and other workers were paid three times more (which they should be; see below), and I accounted for every hospital expense such as building costs, utilities, drugs, and equipment, there was still a significant gap. Where did all that money go? To the bloated hospital administration and its often grossly overpaid leaders.
Many people have a mistaken idea about nonprofit corporations such as hospitals, thinking of them as friendly, benevolent organizations. Wrong! Here's the real difference:
Instead of distributing profits to shareholders (as most corporations do), nonprofit corporations keep it and divide it amongst the top brass, who can be paid well over $1 million per year.
High hospital profits hurt medicine, expert argues
Excerpt: “"Non-profit" hospitals have become extremely profitable, with the non-profit tax exemption estimated at a whopping $24.6 billion in 2011. … Dr. Doroghazi … believes that the executives at "non-profit" health chains have seized some of the tax-exempt advantage for their own personal enrichment, paying themselves millions or even tens of millions of dollars in compensation. So why are such high hospital profits detrimental to medicine?
According to Dr. Doroghazi, "I believe the quest for profits between all hospitals, non-profit and for-profit, has been one of the main drivers causing our health care costs to be the highest in the world, far out-stripping inflation. … I believe current hospital competition has done nothing but drive up costs: new hospitals are often described by locals as a Taj Mahal, with spacious, well-appointed rooms, art work on the walls, and lobbies larger than indoor football fields. Hospitals add high-end, expensive technology that benefits few, and then unleash their Madison Avenue-size advertising budget to tell everyone they are the fourth in the area with a helicopter."”
Comment: Exactly; in the 1990s, I began writing about this deplorable trend. It's sickening.
Once you realize this, it is easy to understand why hospitals are ruthlessly tough on folks who don't promptly pay their bills, which are often fraudulently inflated. By not paying every penny, you are depriving those overpaid hospital executives of luxuries they feel entitled to, such as expensive homes, cars, aircraft, and even women who are drawn like magnets to men with money. Those big shots think they deserve to bleed the communities they purport to serve, so they instruct their bill collectors to be very nasty, heartless, and even needlessly rude and insulting. Collecting money is a war they intend to win, no matter what it takes.
Upset about the strong-arm tactics used against them, patients would sometimes call me at home. I helped them (and many others) out by canceling the part of the bill I could control: the ER doctor charges from my independent contractor group. I did that by giving professional courtesy to patients, even when they weren't doctors—the usual recipients of professional courtesy. That meant we earned less than zero for those patients, since we had plenty of expenses, but I was happy to help them. Surprisingly, my bosses never said a word to me about all the free care I gave away.
Professional courtesy
Most doctors need professional courtesy as much as Bill Gates needs an allowance. While physician professional courtesy is a nice gesture, it would be even nicer to help people with less money and fewer connections. I did that while I worked in the ER, and I still do it today in medicine and elsewhere. For example, I am now selling my Sea-doo, Ski-doo, and shed to help a deported person reenter the United States. I give free firewood to folks in need, and I offered to give some of my inventions away.

While working in the ER, I witnessed how people with money help others with money. I had a very early Christmas one year when a wealthy man I'd recently treated placed a mountain of gifts on my front porch. When I saw it after driving home from the ER, I was stunned. He also gave me an expensive car to use for as long as I wanted. The matriarch of a rich family whose wealth is traceable to oil and related businesses took a liking to me and showered me with gifts and kind notes. I've been offered free food by restaurant owners and given many other freebies, but what I enjoyed most were the nice notes and acts of kindness I received, even ones that cost little or nothing. While it was nice to receive the expensive stuff, I would have preferred that it go to someone who really needed it. After all, what did I need with two cars? Instead of giving free use of a car to a doctor, why not give it to a struggling single mother?
Here's a tip that can save you a boatload of money: When patients enter hospitals, they sign forms authorizing their treatment and agreeing to pay the often-inflated bills. I learned a valuable lesson by watching how some patients would carefully read the contracts, cross out any terms they didn't like, and even add their own terms. The revised contract they signed became the contract. Admitting clerks never contested those changes, so they were legally binding on both parties. Perhaps the hospital could have refused to accept the contractual changes, but realistically they had little power over patients determined to get their way.
What could hospitals do? Refuse to treat those patients? Transfer them? Doing either would subject them to potential liability that made a reduced bill seem inconsequential, so they said nothing and accepted the revised terms.
This inspired me to create a page tutoring people on how to slash their hospital bills. See Want to save money on hospitalizations whether or not you’re insured?
60 Minutes and other investigative journalists have documented the dirty tricks that hospitals often pull on their patients, such as charging for services, tests, medications, and procedures never rendered. This happens so often it can only be explained by postulating that hospitals have incredibly stupid employees (not true) or that administrators create billing procedures that make overcharges and repeated charges more likely and more difficult to detect.
Our legal system gives hospitals a license to steal from patients. If they're caught, they effectively have a get out of jail free card: they must cancel the fraudulent charge, but are not prosecuted for it. This is yet another example of how small-time thieves face harsher penalties than big-time crooks. If you steal a $10 item from a store, you may end up in handcuffs and jail, and pay for that mistake the rest of your life. If a hospital steals 1000 times that much by fraudulently inflating charges, it usually gets away with it because they intentionally make bills so indecipherable that even doctors can't make sense of them.
If the overcharges are detected and contested, the fat cat executives who crafted the shakedown schemes never pay a penalty for them, so they can and do make shoplifters seem like petty criminals. They plunder their communities but get away with murder. If you think that is an overstatement, consider this: high medical costs deter many people from getting the care they need. By not seeking treatment, or by delaying treatment, many people suffer and die as a result. Thus, patients pay a big price for the sky-high salaries of hospital big shots, who make out like bandits by robbing patients.
Why would hospital big shots do that? Don't they care about their communities and the people in them? A few hospital CEOs do, but most have seemingly taken lessons from the Mafia in how to screw people. Although most hospitals are nonprofit corporations, their leaders run them as money-making machines to support their desires to live like kings.
Why aren't nurses paid more?
In theory, Americans live in a capitalistic society in which the laws of supply and demand automatically correct worker shortages. A shortage of nurses should trigger wage increases and other benefits to induce more people to enter the nursing profession, work more hours, and retire later. However, administrators are often determined to preserve the caste system in which they are the royalty and nurses and other workers are the peons. Even if they deserve more, administrators will be damned if they'll give it.
I saw evidence of this in how administrators at a local hospital responded when nurses went on strike with modest demands. Rather than give in to them, administrators fought a protracted battle that cost them considerably more in the end.
This desire to keep nurses down where snobby executives think they belong explains why the local hospital CEO is raking in more money than ever even though some nurses are subjected to significant cuts. It's called priorities. Preserving their country-club lifestyles means much more to them than equitably paying people. Big shots keep nursing wages artificially low because many of them, despite the lip service they give to respecting nurses, think of them as dirt and treat them like dirt. Local nurses who threatened to unionize were targeted with the wrath of administrators, one of whom screamed at them like a deranged maniac.
Nurses and other employees could combat this multifaceted mistreatment by banding together in a massive union with real clout (not just isolated pockets of unionism), but they don't. A nurse friend explained this by saying that nursing students are essentially taught to take it on the chin.
Are hospital CEOs worth it?
Countless times when I performed surgery, I'd take an instrument from its sterile pack, open it, and grimace in disgust as dried blood from a prior patient showered out of its hinge. One day I went through every sterile pack in the hospital that included the instrument I needed, and all had dried blood! Since autoclaving does not eliminate every transmissible agent (such as prions that cause transmissible spongiform encephalopathies—fatal degenerative brain diseases), did the hospital brass express appreciation or at least tolerance for my desire to protect my patient? No, they were livid that I “wasted” so many sterile packs, searching for a clean one! For that they deserved Lotto-sized paychecks?
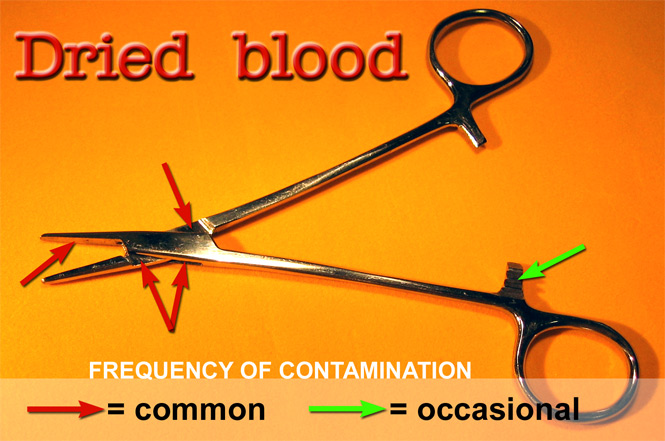
I've witnessed hospital infectious disease horrors that make dried blood seem inconsequential, and countless other patient risks that I repeatedly addressed only to have them fall on deaf ears. Blood injected into a multi-dose drug vial was “no big deal,” a drunk nurse was “none of my business,” and a highly intoxicated mentally ill patient who eloped from the ER at night was someone I should have “just let go” despite prior legal precedents in which courts correctly found that hospitals are obligated to protect patients who are a risk to themselves. This particular woman was so out of control that it took every police officer in the county, along with state police from the adjacent county, to get her into the ER. “Just let her go,” Dr. Einstein? And what should I have told her daughter had she been struck by a car and killed while walking 40 miles home on a moonless night? Sorry, kid?
Some hospital administrators are very bright, ethical people genuinely concerned with patient care, but I've met even more bozos who use inscrutable logic and think the bottom line is more important than doing the right thing.
When one of my bosses expressed patient safety concerns to another hospital CEO, the big shot told him the bottom line was his primary concern. If patients died but the cost of settling possible lawsuits (many medical mistakes are never uncovered) was less than the cost of increased staffing that might avert those problems, he preferred that patients died, likely to help fund his $1.6 million salary, not including benefits and deferred compensation.
The overpaid head of a supposedly Top 100 hospital stunned me by saying he wouldn't fire an unhinged nurse who assaulted a patient's relative (me) who angered him by having the audacity to suggest that my dying Aunt, gasping for breath and complaining of chest pain as she tore at her gown, screaming “I can't breathe! I can't breathe!,” should be given oxygen. Suggesting oxygen for a severely anemic critically ill patient is hardly reason to assault a patient relative, as if anything could excuse such an outburst. This CEO, who looks like the Pillsbury Doughboy™, thought otherwise.
I could fill a book describing other cases that made me question the intelligence and ethics of hospital administrators, so when those unscrupulous rocket scientists say “jump,” challenging them is often better than asking “How high?”
The hospital with the assaultive nurse claims to be so concerned about patients (but not relatives accompanying them?) they are effectively telling employees to get the flu vaccine, or get out. Oh sure, they will accept excuses such as religious objections, but that will just give the hospital cause to find another reason to fire the employee.
Are flu vaccine benefits overstated?
Hoping to mitigate objections to the influenza vaccine, hospitals cite its benefits by pointing to studies demonstrating its efficacy. Not all scientists agree. In fact, some asseverate those studies are overhyped, saying that influenza vaccines have only “a modest effect in reducing influenza symptoms and working days lost. There is no evidence that they affect complications, such as pneumonia, or transmission.” They added:
“Studies funded from public sources were significantly less likely to report conclusions favorable to the vaccines. The review showed that reliable evidence on influenza vaccines is thin but there is evidence of widespread manipulation of conclusions and spurious notoriety of the studies.”

Doing the right thing for patients?
Or getting more money?
Translation? Drug companies are likely up to their usual dirty tricks, paying medical whores to fudge data, overstate benefits, and downplay risks. Supposedly evidence-based research is often hopelessly tainted when researchers are paid under-the-table or otherwise influenced to favorably slant their presentations. For the right price, some doctors and other researchers will say whatever is requested. I was offered a surprising amount of money to favorably write about a product I thought was garbage, so I said no. Other docs are less principled, evidently thinking their desire to be wealthy is more important than the desire of patients to be healthy and happy.
Commenting on the fudged flu data, NaturalNews.com said, “All the hoopla over flu deaths and the need for a flu vaccine are grounded in junk science and faulty statistics.”
“Junk science,” “faulty statistics,” and “spurious notoriety of the studies”—a highly damning phrase. You know what notoriety means: the state of being known for some unfavorable act or quality; infamy, ill fame, dishonor, discredit, disrepute, bad reputation—about what you'd expect from data massaged by medical whores.
spurious (adjective): concocted in order to deceive; not being what it purports to be; lacking validity; not genuine, authentic, real, or true; false, fake, or fabricated; not in accordance with facts or reality; supported by questionable evidence; plausible but false: specious; made-up, fictitious, fictional, deceitful, sham, fraudulent, bogus, mock, feigned, phony; based on pretense: meretricious.
In A scientific look at the missing science behind flu season vaccines, Mike Adams wrote that “flu season vaccines are mainstream medicine's version of psychic surgery: It's all just "medical sleight of hand" based on nothing more than clever distractions and the obfuscation of scientific facts. Flu season shots, you see, simply don't work on 99 out of 100 people (and that's being generous to the vaccine industry, as you'll see below). [... The] implication [that flu vaccines are effective] is wildly inaccurate. In fact, it's just flat-out false. As you'll see below, it's false advertising wrapped around junk science. [...] The vaccine industry … consistently manipulates data, bribes researchers or otherwise engages in scientific fraud in order to get the results they want.” Read the rest of his article
The Cochrane review manifested the chasm of difference between the flu vaccines' marginal benefit and the perception of them by the public and gullible doctors, pharmacists, and “apologist bloggers”: the dupes of the vaccine industry. That efficacy gap would likely be even greater if so much vaccine research wasn't funded by its manufacturers. Cochrane scientists stated:
“Our results may be an optimistic estimate because company-sponsored influenza vaccines trials tend to produce results favorable to their products and some of the evidence comes from trials carried out in ideal viral circulation and matching conditions and because the harms evidence base is limited.”
The Cochrane Collaboration is an independent, not-for-profit large and well-respected organization comprised of world leaders in medicine, health policy, research methodology, and consumer advocacy who advocate evidence-based decision-making. In short, they are a light-year ahead of a local hospital that is pressing the flu vaccine on its staff, hoping they are stupid enough to believe the so-called evidence-based research from medical whores.
Mike Adams summed it up by saying:
“The false advertising of the vaccine industry … implies that if you get a shot you're "protected" from influenza. They claim you won't miss work, you'll stay well, and so on. Through these messages, they are cleverly implying that vaccines work on 100% of the people. But based on the available scientific evidence, these are blatantly false statements. And the wild exaggeration of the supposed benefits from vaccines crosses the threshold of "misleading advertising" and enters the realm of "criminal marketing fraud." [...] Vaccine marketing is, essentially, scientific fraud. To claim that vaccines protect everyone when, in reality, they may reduce symptoms in only one out of 100 people is intellectually dishonest and downright fraudulent. It is, simply put, just pure B.S. quackery.”
I agree with him now, but a few years ago, when I bought the flu vaccine hype and eagerly awaited my yearly vaccine, I argued with a friend who refused to be vaccinated. I graduated in the top 1% of my class in medical school and she never even stepped foot in one, but by keeping an open mind—something not taught to med students—and digging in to this matter à la Cochrane, she was far ahead of most others (as she is in so many other ways) in concluding that influenza vaccines are given an undeserved luster by exaggerated marketing that suggests benefits dreamed up by medical whores not much better than snake oil salesmen.
Adams sagaciously noted:
“That even rational-minded scientists can be so easily hoodwinked by the vaccine industry is causing more and more people to question the credibility of not just modern medicine, but the entire scientific community as well. Because if so-called "rational" scientists and thought leaders can be so easily suckered into an obvious falsehood, what other fictions might they be promoting as fact?”
That hits the nail on the head in terms of capsulizing and explaining my dwindling enthusiasm for traditional medicine. It is far from worthless, but many of its benefits have been oversold. When you add up all of the supposedly miraculous medical advances, you might think that people would enjoy radiant health and live to 120. Instead, I see people in the local upscale tourist town—denizens and visitors alike—who often look like malformed marshmallows with premature aging, have all the zip of a tortoise, and once-in-a-blue-moon smiles. If the medical cure isn't killing us, what is?
Perhaps it is our increasingly abysmal lifestyles and diets. We're careful about the gas we put in our cars, but not the food in our bodies. Doctors are partly to blame for this because they and their apologists promote the notion that the path to health is paved with pills. Dead wrong. I spend about 1000 hours per year studying health. After years of doing that, I found a mountain of evidence indicating the myriad benefits of food. If you utilized that information, you could be much healthier, happier, attractive, slimmer, smarter, and more creative.
In explaining some of the positive vaccine studies, Mike Adams said they originate from “what's known as a "scientific circle jerk" where one group of bought-off scientists quotes another group of bought-off scientists as "authorities" even though they all parrot the same medical quackery of their masters—the pharmaceutical companies.”
In calling the H1N1 pandemic a “false pandemic,” Dr. Wolfgang Wodarg asserted:
“Pharmaceutical companies have influenced scientists and official agencies, responsible for public health standards, to alarm governments worldwide. They have made them squander tight health care resources for inefficient vaccine strategies and needlessly exposed millions of healthy people to the risk of unknown side-effects of insufficiently tested vaccines.”
Circumspect people will not dismiss possible side effects such as Guillain-Barré syndrome (see H1N1 Vaccine Associated With Small but Significant Risk of Guillain-Barré Syndrome based on Risk of Guillain-Barré Syndrome Following H1N1 Influenza Vaccination in Quebec).
Shannon Brownlee and Jeanne Lenzer, two of the world's best medical writers, said “some flu experts are challenging the medical orthodoxy and arguing that for those most in need of protection, flu shots and antiviral drugs may provide little to none.” They also noted that doctors who question flu vaccine efficacy may face professional repercussions.
I agree. Anyone who goes against the grain of conventional standards is often labeled a quack or crackpot. Lisa Jackson, a courageously brilliant physician, ignored that threat and conducted a review that showed “the healthy-user effect explained the entire benefit that other researchers were attributing to flu vaccine, suggesting that the vaccine itself might not reduce mortality at all.”
Brownlee and Lenzer wrote:
“The annals of medicine are littered with treatments and tests that became medical doctrine on the slimmest of evidence, and were then declared sacrosanct and beyond scientific investigation. In the 1980s and ’90s, for example, cancer specialists were convinced that high-dose chemotherapy followed by a bone-marrow transplant was the best hope for women with advanced breast cancer, and many refused to enroll their patients in randomized clinical trials that were designed to test transplants against the standard—and far less toxic—therapy. The trials, they said, were unethical, because they knew transplants worked. When the studies were concluded, in 1999 and 2000, it turned out that bone-marrow transplants were killing patients.”
Who is the quack?
Excerpt: [They were fined in part for] “failing to report safety data about a top diabetes drug.”
Article: Discrepancies in clinical trial reporting raise questions of accuracy
Excerpt: “In an analysis of 96 research trial results published in top journals, almost all had at least one discrepancy between what was reported on the public clinical trial registry clinicaltrials.gov and what was posted in the journal article. A new research letter raises serious questions about the accuracy of results reporting in both clinical trial registries and publications …”
Article: Japanese Superfood Prevents Flu Infection
Comment: Don't you just love those active Japanese minds?
Article: Scientists identify 'decoy' molecule that may sharply reduce risk of flu death: Molecule protects body from dangerous overreaction to viral attack
Article: Vitamin E may prevent pneumonia in nonsmoking elderly men
Article: Lactic acid bacteria can protect against Influenza A virus, study finds
My faith in medical research is tempered because pharmaceutical companies often cherry-pick results to make their products seem more beneficial and less risky than they really are. Dr. Mitsuyoshi Urashima said that “vitamin D was more effective than vaccines in preventing flu.” So why aren't hospitals requiring their employees to obtain optimal amounts of vitamin D?
We used to think of vitamin D as a calcium regulator, but it functions as a hormone with a finger in many pies, not just mineral metabolism. A mountain of evidence suggests that activated vitamin D has myriad beneficial effects, including “profound effects on human immunity” and reduced “risks of cancer, heart disease, diabetes and other illness, including various bacterial as well as viral infections.” A physician who extensively reviewed the vitamin D scientific literature stated:
“New research suggests that influenza is also a disease triggered by vitamin D deficiency. Influenza virus exists in the population year-round, but influenza epidemics are seasonal and occur only in the winter (in northern latitudes), when vitamin D blood levels are at their nadir. Vitamin D-expressed genes instruct macrophages, the front-line defenders in the innate immune system, to make antimicrobial peptides, which are like antibiotics (Science 2006;311:1770–1773). These peptides attack and destroy influenza virus particles, and in human carriers keep it at bay.”

sunshine strikes bare skin
Since at least half the people in the world are deficient in vitamin D and few have optimal levels of it, why are hospitals pushing flu vaccines but not vitamin D? They profess to care about their patients and staff, yet they ignore or give short shrift to vitamin D that can help people in ways that vaccines cannot. Any hospital that mandates flu vaccines but not vitamin D is unconscionably negligent, led by people with more power than brains.
Can you guess why hospitals, the government, and drug stores push vaccines, not vitamin D? Even if you believe that the vaccine merits outweigh its risks, there is something very fishy about this. Why are they giving so much emphasis to the vaccine (which may or may not work, depending on how accurate scientists are in forecasting what influenza strains to target each year) and little to none regarding other preventive measures, such as vitamin D, that are safer and boost protection against many infectious diseases besides flu?
Vitamin D works every year, not just some years. A healthcare worker with optimal vitamin D is less of a risk to patients. Vitamin D can essentially add another layer of protection beyond that offered by the flu vaccine, so hospitals should not ignore it. That vitamin becomes a hormone in the body that can make the difference between life and death, so ignoring or trivializing it is just plain stupid.
If parents were similarly hyperfocused on one bit of advice, they might caution their children to not accept candy from strangers, but say nothing about looking both ways before crossing a street. What would the government call such parents? Irresponsible and perhaps even criminally negligent. Oddly, the government sanctions this myopic focus on protecting against the flu by using the vaccine but says little or nothing about the dozens of other ways people can minimize their risk of acquiring myriad other infectious diseases.
What is the best way to explain this lack of expertise on the part of experts? By postulating that they are not as intelligent and informed as they are presumed to be? That they are selectively book-smart but lack common sense? Or by assuming they have an ulterior motive for their multiple glaring errors of omission?

Some vaccines are a godsend, but I am troubled by their recent massive emphasis. With the way the government and big businesses are touting them, one might think that vaccines were even more essential than vitamins. It is bad enough seeing drug stores proudly announcing they give vaccines every day of the year (“Hey, Mom, let's go get our Christmas vaccine!” :-), but in a clothing store in the middle of summer, I was shocked to see a “Get your vaccine here!” table in the middle of racks of shirts, sweaters, dresses, and pants. What's next? Putting a mini vaccine clinic in McDonald's playrooms so kids can slide down those colorful plastic tubes and be met by a nurse with a big smile and even bigger syringe?
Vaccines have historically done some good, but part of their reputed benefit in terms of preventing disease actually resulted from improved sanitation regarding our food, water, and waste.
When people in power do things that leave the rest of us scratching our heads in befuddlement, consider the motivations that drive big shots: money, power, and sex.

Blah, blah, blah … who cares? You should, because such astoundingly gorgeous women usually don't work for peanuts. The money in her fat paychecks, and the money that paid for the food I barely noticed, ultimately came from consumers like you who paid too much for your prescription drugs.
A pharmaceutical company paid a gorgeous drug rep to take me out to a nice restaurant. Just me and her. There wasn't any education about her drugs (the usual excuse given by drug companies), just a bold-faced attempt at making me think this free lunch with a goddess would foster a sense of obligation to prescribe their latest antibiotic. Top drug reps can earn more than doctors, so they have an incentive to influence doctors any way they can. If sex doesn't sell, why are pharmaceutical manufacturers eager to hire cheerleaders? Their brains, or their bodies?
“Drug reps often have no medical or science education,” but oh, are they ever yummy! When my older brother attended a training seminar populated by the usually attractive cell phone sales reps, he was stunned by how much more attractive the attendees were in the adjacent room: they all appeared to be gods or goddesses. You guessed it: they were drug reps in training.
Testifying before Congress, Shahram Ahari, a former pharmaceutical representative, indicated that “drug companies like hiring former cheerleaders and ex-models to wine and dine doctors, exaggerate the drug's benefits and underplay their side-effects.” He said his job involved “rewarding physicians with gifts and attention for their allegiance to your product and company despite what may be ethically appropriate.” He added they use “friendships and personal gifts to foster a "quid pro quo" relationship, and how to exploit sexual tension.”
And how!
Being only an ER doctor, I got nothing but a free lunch and a chance to gaze into one of the most mesmerizingly beautiful faces I'd ever seen. What about people with real power, such as hospital CEOs, who dictate what thousands of employees and doctors do? Might a chance to sell a truckload of vaccine make some drug reps willing to do more? An ex-girlfriend, one of the few Plain Jane drug reps, said the hot babes she'd worked with earned more money by being more than friendly to bigwigs. I found that difficult to believe, but businessmen and politicians have been bribed with sex and other under-the-table inducements.
Yet another drug company dirty little secret

Pharmaceutical representatives have access to a database that tells them how often a specific doctor prescribes various drugs. I didn't learn of this secret database until I'd been a doctor for a decade. While chit-chatting with a drug rep friend and neighbor (whose home was much nicer than mine—know what that means?), he told me about it. I was shocked. My prescribing habits are none of their business, yet they milk that data (and sell it) to know which doctors to target and to gauge the effectiveness of their efforts.
Thus, the drug rep goddess mentioned above may have thought to buy a meal for me based on my prescribing habits. Once doctors figure out that prescribing more of an expensive drug can earn them one-on-one time with female drug reps who look like supermodels, doctors are more likely to prescribe the drugs. Drug companies aren't stupid; they know that spending money this way boosts their profits even after deducting expenses for meals (and whatnot) and handsomely paying their super-attractive reps.
If the bats in the doughboy CEO's belfry tell him not to axe a nurse who behaves like a thug, there's no telling what other insanity might flow from his second-rate mind, such as mandating flu vaccines but not vitamin D, which is just the tip of the preventive health iceberg. In the doughboy's twisted mind, it is OK to threaten an employee for not giving in to his vaccine demand, but not acceptable to fire a nurse with an impossibly short fuse. Go figure. The doughboy wouldn't even accept my suggestion to compel the nurse to get anger-management therapy. Nuts.

The risk of acquiring and possibly transmitting infections, not just influenza, is minimized by good nutrition (not the junk most Americans eat), not smoking, obtaining sufficient sleep, and stress mitigation. Perhaps some hospital somewhere cares about the sleep and stress of its employees and doctors, but every hospital I've worked in—from prestigious ones affiliated with a medical school to a Yuppie Town USA hospital to a friendly, hometown one in Nowhere USA—didn't give a hoot if their employees smoked like a smokestack, spent nights drinking in a bar instead of sleeping, and ate food that made fast food seem downright healthy.
Most hospitals feed their patients and employees nutritionally third-rate food such as French fries, soft drinks, potato chips, bacon, hot dogs, Jell-O, white bread and pasta, cookies, cakes, pies, artificial creamer, and loads of artery-clogging trans fats, even to cardiac patients. Hospitals should set a good example of healthy eating, but they don't, even when it can make the difference between life and death. Their doctors and dieticians evidently don't keep up with the latest research, such as that showing how substances other than vitamin D can also enhance immunity. One is quercetin, which protects against influenza. Thousands of other healthy food choices can help people in myriad ways so they feel and look better, recover more quickly from illness, and have less chance of future disease. Hospitals ignore this because they either don't care or know enough, even though it is backed by research from scientists who have nothing to gain by fudging data, as is commonly done with prescription drug research. I spend about 100 hours per month keeping up with that research, which is evidently too much for hospitals to keep current with. They'd rather fill their patients with crummy food and pills, which is great for the processed food and pharmaceutical industries.
Thus, when I hear hospital big shots professing to care about the health of their workers, I wonder if they even know what health is. Judging by the bloated body of the aforementioned doughboy CEO, the answer is a resounding “no.”
Why would anyone with an ounce of common sense follow health advice from someone with premature aging who looks like death warmed over and acts like a graduate of a Nazi charm school? Whatever he's selling, I'm not buying unless someone with a functioning brain explains why they have the legal and ethical right to mandate influenza vaccines but not things less risky and more beneficial. I could (and will) fill a book presenting hundreds of ways to minimize the risk and duration of infections such as colds and the flu. Hospitals and even the CDC (which has all the time in the world) focus on a few infection-control measures while ignoring most of them.
The myopic focus on the flu vaccine suggests hospital bigwigs are either utterly unconcerned with optimizing patient and staff welfare, or they are too ignorant to know better. So, big shots, do you not know what you are doing, or do you not care?
Hospital administrators who mandate influenza vaccines remind me of Army generals with early dementia who fortify one defensive position yet leave others wide open to attack. The doughboy CEO's hospital has a very liberal visitor policy: anyone can visit any time of the day or night, whether or not they received the flu vaccine. I've visited relatives on days when visitors outnumbered the staff. Consider this: Germs don't spread only from hospital workers, of course; visitors can spread them, too. Everywhere I looked, I saw visitors: some sneezing, some coughing, some wiping their noses, and so forth. While walking with the hospitalized friend or relative in the hallway or even room, visitors passed within inches and sometimes even touched, thanks to annoyingly small rooms and hallways.
Furthermore, the hospital will, of course, accept unvaccinated patients, who can spread germs to other patients.
A germ is a germ, and a human is a human. Therefore, insisting that workers but not visitors or patients be vaccinated is like spraying mosquito repellent on one half my body but not the other.
If hospital administrators have the right to threaten employees with the loss of their jobs, don't employees have the right to insist their leaders make logically consistent decisions? Only Martians would think it is permissible to stress the influenza vaccine but not other things that can do much more for workers and patients.
The influenza vaccine is not without risk, and the risks we know may be minimized by companies with a vested interest in cherry-picking results and bribing government officials and doctors to echo their slanted views. Remember what Shahram Ahari said? They “exaggerate the drug's benefits and underplay their side-effects.”
The revolving door between drug companies and the FDA is not surprising; our incompetent government thinks that getting in bed with Big Business and Big Pharma is just another day (or night) in Washington, DC. One of my relatives, President Chester Alan Arthur, earned the moniker “The Father of Civil Service” by signing the Pendleton Civil Service Reform Act into law, which replaced the spoils system with a more equitable one. Modern Presidents and Congress turn a blind eye to the incestuous relationship between the FDA and pharmaceutical companies, which Arthur surely would not tolerate.
“Guillain-Barré syndrome remains the most frequent neurological condition reported after influenza vaccination to the Vaccine Adverse Events Reporting System (VAERS) since its inception in 1990.” The Guillain-Barré syndrome is serious and sometimes fatal. If you die or suffer permanent disability from a vaccine you were coerced into getting, shouldn't you or your family be able to sue the hospital that twisted your arm? If your hospital (or other employer) compels you to receive the flu vaccine as a condition of continued employment, will they pay your workers' compensation benefits if you have an adverse reaction? Legal precedent holds that job-related injuries are covered, thus making your employer liable.
A 2003 retrospective study strongly suggested that Franklin D. Roosevelt's paralytic illness was caused by the Guillain-Barré syndrome, not poliomyelitis. If you must spend the rest of your life in a wheelchair like Roosevelt, watch the doughboy or his equivalent at your hospital squirm in his chair as your lawyer grills him.
Vaccines are not without risk. India suspended its Gardasil vaccination program when “4 girls died and 120 were injured after receiving the vaccine.” Its potential complications are severe and even shocking.

Who will take care of your family if you die or are disabled by the vaccine? Will the millionaire doughboy invite them into his expansive home or even dog house? Fat chance of that, but it is a question every hospital CEO should answer before he or she demands that even one employee risk his life by receiving a vaccine that almost certainly won't kill you—but it might. Guillain-Barré syndrome and other flu vaccine risks should be carefully considered by every potential recipient, not by Big Brother and his daffy sidekicks—like the doughboy CEO—who are increasingly demanding the right to think and decide for you. I experienced nightmarish problems by taking FDA-approved drugs made to seem as harmless as M&M's® by drug companies eager to make a buck. I could not begin to count the patients I treated with problems caused by prescription drugs, not natural causes.
How can hospital CEOs with business degrees and no great ideas truly deserve to be paid several times more than doctors? Earning a medical degree and medical license is considerably more challenging than obtaining a business degree. Leonard Mlodinow, author of The Drunkard's Walk: How Randomness Rules Our Lives, wrote a fascinating and provocative article entitled The Meritocracy Paradox for Forbes magazine that discussed how hotshot CEOs are often just the beneficiaries of luck, not everlasting talent. This explains how hospital CEOs with lackluster minds can fall into positions they deserve as little as their gold-plated salaries and benefits. All too often, they are not brainiacs, just leeches who know how to milk the system. If they have The Right Stuff, let's see it.
Like other tyrants, hospital big shots have easy solutions: just crack the whip and your employees will behave. They could order staff to clean stethoscopes, pens, and computers after every use and to change their uniforms the minute they're contaminated, but most hospital personnel are already working at a breakneck pace that itself endangers patients. Adding more responsibilities without more staffing will only increase the burden on employees who are already shouldering more than they should. If hospital leaders deserved their immense incomes, they could think of ways to improve system efficiency so their staff could do more in less time. Instead, workers struggle to deal with stumbling blocks erected or approved by administrators, such as computerized medical record systems that waste staff time.
If CEOs cannot think of how to improve the system, something's got to give. I suggest eliminating their fat paychecks and using that money to hire more people to do work that clearly needs to be done. The CEOs will agree, because patients are their primary concern, correct? Surely they are more important than living high on the hog, right?
We'll see.
I have a suggestion for hospital CEOs: get off your high horse, stop puffing out your chest, and address every concern from workers and medical staff who think you're overstepping your legal and ethical authority. Explain why you are so impressed with the influenza vaccine but not infection control measures that are safer and could do more for more patients. Cite the legal precedent or logical principle that justifies you acting like a Nazi about the flu vaccine but an irresponsible teenager on other, even deadlier infections. If you are worth what you are paid, answering such questions should be easy. If you don't respond or are evasive, the community you feed upon like a parasite should search for someone more qualified, with a better brain and a bigger heart, who is more concerned with patients than living like a king.
Patients truly are Number One, so let's give them everything they deserve to be healthy. If that requires a hospital CEO to live like a prince instead of a king, so be it. As Leonard Mlodinow suggested about CEOs in general, hospital big shots are often just the beneficiaries of luck, not talent or brainpower. If hospital hotshots think their luck entitles them to live like kings, they're living in a dream world. The rest of us, who live in the real world, know that health is more important than the expensive CEO toys that add so much meaning to such empty lives.
The Dunning–Kruger effect explains why hospital CEOs (and many others) overrate their abilities, producing illusory superiority.
Yet another danger of the influenza vaccine
German philosopher Friedrich Nietzsche said, “What does not kill me, makes me stronger.” As a corollary to this, he might have said, “What protects me makes me weaker.” In other words, standing on our own two feet and facing the cold, cruel world, getting some figurative bumps and bruises along the way, can strengthen us. This calls to mind a relevant saying, “The hottest fires forge the strongest steel.”
If that is too allegorical for you, just remember that adversity can strengthen you. That is certainly true of the immune system, too. Babying it can weaken you, making you less able to successfully combat future infections, possibly giving you more complications or even a shortcut to the grave.
Scientists published a paper in the Journal of Virology, Annual Vaccination against Influenza Virus Hampers Development of Virus-Specific CD8+ T Cell Immunity in Children, that ought to send chills down the spine of anyone bright enough to understand it. Lead author Dr. Bodewes said that “annual flu vaccines … could leave people more vulnerable to novel pandemics.”
Influenza pandemics are nothing to sneeze at. They “occur when a new strain of the influenza virus is transmitted to humans from another animal species,” producing “an epidemic of an influenza virus that spreads on a worldwide scale and infects a large proportion of the human population. In contrast to the regular seasonal epidemics of influenza, these pandemics occur irregularly, with the 1918 Spanish flu the most serious pandemic in recent history. Pandemics can cause high levels of mortality, with the Spanish influenza estimated as being responsible for the deaths of over 50 million people.” [source]
A highly pathogenic virus variation will eventually emerge, perhaps causing even greater mortality. Predictably, the ones most likely to die will be the folks who thought they were doing themselves a favor by being vaccinated each year.

“Only” suggests it is a real bargain.
Perhaps not.
Where's the prescription?
Many states permit pharmacists to give vaccines without a prescription. Influenza vaccines are certainly drugs, with risks and benefits no less serious than those of other drugs that could land pharmacists in prison for years if they dispensed them without a valid physician order. Frankly, most doctors don't know enough about the flu vaccine to adequately give informed consent about it, but you might be lucky enough to have a doc who explains its pros and cons. If you walk into one of the big pharmacy chain stores, what is the chance of receiving similarly personalized, detailed information? Probably close to zero. Their desire to profit from you is likely greater than their desire to educate and protect you. If they put you first, they would tell you about vitamin D and other things that minimize your risk of influenza and other infectious diseases. But do you get all that? No, you get deafening silence other than the cha-ching of a cash register tallying another flu vaccine sale.
A wise internist noted, “the [pharmacy] profession is now trying to extend its reach, and gain modern relevance, by trying to take over medical functions at the margins. But this behavior may not be safe.”
A flu vaccine risk
Influenza vaccine recipients often acquire a false sense of security, as if marginal protection from the flu confers a magic shield to protect them from other infectious diseases. As a result, they let their guard down, fail to take commonsense precautions, and consequently get sick more often.
Based on my limited experience seeing hundreds of thousands of people in the past few decades (which is anecdotal but a sample large enough to be statistically significant for my informal observational study), as more people get flu vaccines, more people than ever get sick during the winter.
For example, I walked in a store in early January and was horrified by what I can best describe as a mass chain reaction of sneezing and coughing. After years as an ER doctor and even after working in a pediatric ER, I've never seen anything like that—but I transitioned to a different medical career before the flu vaccine mania hit big time. Mind you, this was a big-box lumber warehouse, not a store selling essential items that people can't postpone purchasing until they're well.
In another article, I mentioned how some young people died from infectious diseases, perhaps because receiving a vaccine gave them a false sense of security.
My advice: think of a vaccine as an insurance policy filled with lots of loopholes. You may be covered or you may not, but even if you are, you certainly won't be for anything except what it is intended to protect against.
Connecting the dots and solving a mystery
I once was a veritable cheerleader for the flu vaccine, but there is now enough evidence to question its efficacy. It certainly has been oversold and is much less effective than it is purported to be. In contrast, the evidence for vitamin D is stronger and more creditable; pharmaceutical companies have no incentive to extol it, so their medical whores have no reason to magnify its benefits and minimize its risks.
Now consider this: if your local hospital is compelling its staff to receive the influenza vaccine but not vitamin D, are they truly up-to-date or do they have a bumper-sticker level of understanding? Do they truly know what they are doing, or have they only enough mental capacity to absorb the drug company talking points? If you put 2 and 2 together, the answer is obvious: hospitals that push flu vaccines but not vitamin D are institutions woefully behind the times, led by people with second-rate minds.
One cannot become a licensed doctor without acing college and the MCAT before passing medical school and licensing exams. There are no comparable hurdles to becoming a hospital administrator, so while they may later acquire the power to tell doctors what to do, they often have more power than brains—a very dangerous combination.
Comprehending this gap between administrator power and brainpower helps solve the mystery of why hospitals make so many mistakes year after year. I've brought obvious problems to their attention—such as a drunk nurse—only to be told that it was none of my business. Whose business is it, then? That nurse didn't just have booze on his breath, he would sometimes intentionally contaminate surgical sterile fields. Was he a malicious sociopath getting a thrill by harming patients? I don't know, but he clearly was a risk to patients. He'd been hired after being fired by GM for repeatedly drinking on the job. I've heard the UAW protects such boozers, so the ones dismissed must be real problem cases. And he was—but the administration didn't want to listen. Who wants to be treated in a haven for GM rejects? Anyone?
Anyone with a room-temperature IQ and an ounce of common sense would not sweep such a problem under the rug. It isn't surprising that administrators who ignore such glaring dangers also ignore less obvious ones, but with healthcare being what it is, even those lesser problems can and do result in patient injury and death.
Patients often go into hospitals only to be given new problems and worries. I went to the local supposedly Top 100 hospital worried out of my mind because I had signs and symptoms of a neuroendocrine cancer. The last thing I needed was another worry, but that is exactly what that Top 100 hospital gave me. Their phlebotomist either didn't know about germs or didn't care. If he screws up while drawing blood from a doctor, he likely repeats his mistake on others.
Drawing blood is about as basic as it gets. It is a routine procedure so simple that even kids could be easily trained to do it on people like me, with a prominent antecubital vein. Hence, if a supposedly Top 100 hospital has an incompetent phlebotomist, what other horrors might patients face there? Plenty, as I discovered (read about one of them).
I accompanied a friend who asked that I serve as her patient advocate during a transvaginal ultrasound in this same Top 100 hospital, and I was horrified by the ultrasound technician's multiple mistakes.
A radio talk show host bitterly complained about how doctors at the local Top 100 hospital repeatedly missed chances to tell him that the high-dose Motrin he took (800 mg three times daily) delayed his healing. On October 4, 2010, ScienceDaily published an article entitled Surprise: Scientists Discover That Inflammation Helps to Heal Wounds. That was no surprise to me. I figured it out years ago and discussed that in my book, Fascinating Health Secrets, published in 1996. The ScienceDaily article was based on research published about a year ago, so the local behind-the-times doctors should have learned of that study by now. However, when you're #1—or think you are—why burn the midnight oil keeping up with medicine? By doing that and thinking logically (instead of blindly accepting what drug companies say), I figured out many things before mainstream medicine and science woke up.
I could, and will, write books revealing many of the minor-to-major mistakes hospitals make, many of which haven't been covered by the media. Together, those errors add up to a mountain of suffering for patients and their families along with extra medical bills that are helping bankrupt our country and people in it. I've seen lives shattered in Top 100 hospitals too busy patting themselves on the back and too concerned about showering their CEOs with money instead of using it to address glaringly obvious problems.

Details were obscured to protect his identity.
Here's a photo of a surgeon wearing scrubs riding a kid's bike going to work.
You don't even need to be treated by a hospital to be imperiled by it. The second-rate minds leading the local Top 100 hospital demand their employees and doctors receive flu vaccines, but not follow even more basic infection control measures. For example, they permit employees to wear uniforms donned at home, thus helping spread germs from there into the hospital. That's less of a concern than what happens when workers leave the hospital, spreading germs into the community that help transmit drug-resistant superbugs. Hence, when you sit down to eat in a restaurant, you may eat in a booth vacated seconds ago by a hospital worker wearing his or her uniform. Betsy McCaughey, former lieutenant governor of New York state, a fellow at the Hudson Institute and chair of the Committee to Reduce Infection Deaths, discussed this problem in a Wall Street Journal article: Hospital Scrubs Are a Germy, Deadly Mess. Related article: Study shows nurses' scrubs become contaminated with bacteria in hospitals: Antimicrobial fabrics are ineffective for preventing transmission (based on The Antimicrobial Scrub Contamination and Transmission (ASCOT) Trial: A Three-Arm, Blinded, Randomized Controlled Trial With Crossover Design to Determine the Efficacy of Antimicrobial-Impregnated Scrubs in Preventing Healthcare Provider Contamination).
Laundering hospital uniforms at home or in a laundromat is risky. Germs are usually just diluted, not thoroughly killed. That is especially true in the case of top-loading washing machines in which contaminated water can splash and adhere to the undersurface of the top lid and other locations from which it may drop onto the current load toward the end of its cycle, or a subsequent load. In a laundromat, those clothes may belong to an unsuspecting person, who could be infected. The water temperature in residential or laundromat washing machines may not be hot enough to kill dangerous bacteria.
At the end of a shift, even uniforms with no visible contamination are still teeming with nasty germs. The brainiacs in charge of the local Top 100 hospital either don't know of this Healthcare 101 problem, or they don't care. In either case, they are incompetent and need someone to knock some sense into their heads. Better yet, they need to step aside so someone more qualified and caring can take their place. When they are too ignorant, stupid, or lazy to address even very basic, obvious problems, do they have what it takes to recognize and solve more esoteric ones?
I propose that we stop putting Band-Aids on problems and address their root causes, such as administrators who won't wake up until they're given a pink slip. If they are too comfortable in their jobs to protect the communities that make them so rich, it is time to clean house.
Ms. McCaughey's Wall Street Journal article appeared January 8, 2009—almost three years ago. The asleep-at-the-wheel doughboy in charge of the local Top 100 hospital has had more than enough time to address this problem, but he appears to be too busy counting his money, playing with his toys, and schmoozing with the board filled with folks who cannot spot a clearly incompetent CEO.
One of my friends was a member of Al Gore's staff when he was Vice President. Her job mandated that she accompany him everywhere, so she went to the White House and attended meetings with him and President Clinton. During one meeting, Clinton was yukking it up so much that Gore lost his patience, screaming at him to “Get with the %*@%#&^ program!”
I have a similar message for the board at the local Top 100 hospital. Unless you want the community to think you're too illiterate to read the Wall Street Journal or other publications with the same message, you should light a fire under the doughboy or, better yet, fire him. If you don't, you likely will wish you did once my book on him comes out. Your Top 100 hospital killed one of my friends, injured me, and hurt many others I care about. Giving your brass a pass would be simply unconscionable.
While working in the ER at a major downstate hospital, I've witnessed the incestuous relationship between hospital administrators and the board. If a board member or other VIP came in, a top administrator would often notify me even before the patient arrived. (Do they have each other on speed dial?) The administrator laid out the red carpet to ensure the big shot board member or VIP received perfect, expeditious care. The administrator would hover over the chart like a mother hen and rush the bigwig's blood or urine to the lab—funny how they'd never lift a finger to help when the ER was stacked to the rafters and patients were moaning in the waiting room and halls. Oh, but we all know top administrators would never touch lab specimens from common people, even if you wore gloves—something they never did for the big shots. Hmmm … .
If the big shot required admission and the hospital was full, the administrator always immediately found a room by ordering staff to discharge someone. That sudden vacancy would be filled by the big shot, never a common person who may have spent the last couple of days on a gurney in the hallway. Whatever happened to first-come, first-served? This was no triage of medical necessity; this was blatant favoritism. Big shots matter and get first-rate treatment; ordinary folks get to use the bedpan in a hallway as strangers walk past.
It didn't take me long to realize why administrators were so attentive to board members or their family: because the board set their salaries and other compensation. By giving the board such exemplary care, they prevented it from experiencing what others receive.
Anyone smart enough to sit on a hospital board should be sufficiently intelligent and caring to not stomach this preferential treatment, but it is just part of how the elite take care of each another while giving commoners the cold-shoulder.
A message to the board
Thus, when I see local talk show hosts extolling your Top 100 nightmare, I think they haven't spent months as I did digging into the hospital award racket, which I concluded was a clever scam in which awards can be purchased—indirectly, of course, for obvious reasons. Or perhaps they've been given VIP care and certainly not the mistreatment I received when one of your Top 100 nurses struck me while my Aunt was dying.
After you investigate how your doughboy CEO mishandled that, and after you see how he lets even glaringly obvious problems persist, you need to get with the program, do your job, and hire a CEO who is worth the fortune you're paying the incompetent doughboy.
Despite strong coercive efforts in 2010, almost half of your employees refused to receive the flu vaccine. If you think about this logically, only two conclusions are possible:
- Those people had valid reasons for rejecting the vaccine.
- Your staff are not as intelligent and educated as you claim.
The second alternative seems untenable considering how you rave about your staff. They are your hospital; the bricks and mortar, machines, drugs, and whatnot are nothing special. People make or break a hospital, and many of yours opted not to receive a free influenza vaccine in spite of strong and repeated pressure. Without that arm twisting, likely over half would have rejected it. So, brilliant members of the board, what plausible reason could explain why so many healthcare professionals said “no”? Is it what we doctors might euphemistically refer to as supratentorial dysfunction? Or might your staff have valid reasons for rejecting the vaccine? In either case, it is a public relations nightmare for your hospital, which is either chock-full of idiots, or led by idiots so bereft of scruples they have no qualms about compelling many smart, informed people to receive a vaccine they have valid reasons for refusing. So who are the idiots? Your employees or your brass?
I'd guess the latter. They swallow the drug company propaganda hook, line, and sinker along with your second-rate infectious disease physicians. Smarter, better educated people listened to the drug whores espousing flu vaccines and concluded they were overselling their benefits almost as wantonly as snake oil salesmen did a century ago.
Since your hospital is the only one in town, people who don't know what a truly topnotch one is are inclined to overrate it, perhaps after hearing the incessant praise from local talk show hosts who also don't know better. I've worked in hospitals that gave vastly superior care—care that often meant the difference between living and dying—so I know how your hospital falls short in many ways.
Why don't more doctors speak up?
When even Top 100 hospitals give horrific care and endanger their communities, why don't more doctors speak up? A very few courageous ones do, but others are cowered into silence because they need a job.
Consider the case mentioned above in which the hospital CEO said his concern for money exceeded his concern for patients' lives. That is very newsworthy, so if my boss were willing to go public with it, local reporters would cover it, and the hospital board would be forced to fire the CEO, who is likely one of their golfing buddies. The elite hobnob together, ya dig?
My boss would be branded as a troublemaker, so they would find an excuse to fire him, or even to replace his group (many emergency departments are staffed by a group of independent contractors, not hospital employees). Not only would my boss be out of a job, his reputation as a whistleblower would make it difficult or impossible for him to find another ER job.
I repeatedly presented various patient safety concerns to top administrators only to have them tell me they weren't interested. I was stunned. Why wouldn't they be interested in patients and visitors being exposed to the HIV virus in a way that could very well infect people? We had an HIV+ patient who wanted the world to die when he did, so he was on a mission to infect as many people as possible. He told me of the hundreds of women he slept with, hoping to infect, and other ER staff said he would go to the hospital cafeteria and intentionally drool on silverware.
One day he disconnected his IV and walked through the public areas of the hospital, dripping a trail of blood. A nurse told me about it even though he wasn't my patient; the other ER doc simply didn't care. I did, so I followed the blood trail and found him. I asked him to return to the ER, but he refused. I offered to buy a pizza for him if he returned, but he wasn't interested. I tried to appeal to his sense of morality by pointing to all of the visitors on this busy weekend day, some of whom would be surely exposed to his blood, which formed a red trail that made me think of the breadcrumb trail in Hansel and Gretel … but this surely wasn't Hansel, and it surely wasn't bread. My primary concern was that one of the many children I saw would inquisitively touch it, as kids are prone to do, and then touch their mouth or eyes. The patient coldly replied that he hoped they did just that, adding, “Fuck 'em all! I hope they all die!”
“But they're just innocent children,” I said.
He told me he didn't care. The younger, the better, he explained. Younger ones have more years of life to lose.
The nurses were able to coax him back (without pizza, I might add), but they refused to restrain him even after he left again to paint another blood trail. The security guard refused to touch him, so the patient had his way, spending his afternoon doing his best to infect as many people as possible.
The administrators who loved the local community (or so they wanted everyone to believe) weren't interested in hearing about this case or how similar ones in the future could be handled better.
I could fill a book describing other cases in which administrators had a clear duty to get involved, but didn't. They are never personally sued; it's always the fault of the doctor or nurse, even when the doctor and nurse are doing their best to deal with problems caused or ignored by administrators who don't care. I had many patients of my own to take care of on the HIV rampage day, and with staff refusing to follow my orders, there was a limit to what I could do. (Incidentally, had this happened in Detroit, one of their police officers would have quickly ended that situation.)
Flash-forward a few years, and one of my relatives was being born in that hospital. However, she was born too late because the moronic administrators had a policy that only doctors could deliver babies, so if anything went wrong, they could blame it on the doctor. Trying to follow this order, the obstetric nurse pushed hard on the child's head to delay delivery until the doctor arrived 15 minutes later. When the child appeared, her father told me that she was dark purple—almost black. The child suffered a brain injury that will ruin her life, and the nurse knew it. She ran into that family a year later and told them how sorry she was for what she did, which she felt compelled to do because of administration pressure. Her father tried to sue but the staff had whitewashed the chart, making the delivery seem routine and uneventful. Just fudge the chart, as drug companies do with data.
Now the scary part. I was just one of several hundred doctors at that hospital. The many botched cases I knew of were surely just a small fraction of their total screw-ups. This wasn't some backwater hospital, but a large, university-affiliated teaching hospital situated in an area that drew plenty of upscale people, including world-famous sports stars and celebrities. So there I was, doing my best to take care of ER patients while battling administrators and patients like the HIV assassin. The pay was great but the stress was off-the-scale, so most of the experienced ER docs we hired said it was too much and quit after the first week, with many lasting just one shift. I stayed for years longer than I should have, then moved up north and found hospitals there to be infected with a wholly different brand of insanity, but one just as lethal to patients.
One of my bosses was so handsome and so well-connected in the community that they didn't spot his incompetence, such as crossing his arms and waiting for a critically ill child to die instead of doing everything possible to save his life (I walked in on this case at the beginning of my shift and was so alarmed by what I saw that I took charge of the case without asking; I saved the child's life, as I described in another article on narcissistic leaders). Was my boss grateful?
Hell, no! Who wants a hotshot downstate ER doctor taking over a case and making the boss look like the incompetent fool he was?
In my ER career, I've seen so much wrongdoing that I had to write about it. One of my comatose patients was gorgeous and likely raped by an ER tech. My other cases (not all focused on malfeasance) were so interesting that I've had several offers to turn them into a new TV series or Hollywood movie. In fact, the director of one of the biggest Hollywood blockbusters of all time contacted me (unfortunately around the time my Mom was dying), hoping to use my true ER stories.
However, there is a drawback to writing: people who focus on problems and write well enough to attract a national audience (as I do) attract attention from opponents who use every dirty trick in the book to make them look bad. They've hacked into one of my websites and changed my words, threatened me, and done their best to marginalize me by taking my words out of context and twisting them to make it appear I said outrageous things I never said.
Here's an example: one organization known for its outrageous smears claimed I wrote that Native Americans “should have been grateful for their subjugation by whites.” That's absurd. I am part Native American, and I strongly condemned that subjugation in writing (in one of my books and websites in addition to this blog) long before I learned of my Native American ancestry. In fact, I don't think any professor or liberal could do a better job than I did in manifesting why that subjugation was a moral abomination. The Trail of Tears means nothing to most people, but it (and events like it) aroused a burning desire in me—even before I knew I was part Native American—to bring those injustices to light, not sweep them under the rug. If you read what I wrote on that subject, you would see that the smear merchants could not possibly have been more wrong.
However, the smear merchants know that most people are too lazy to check if what they write is true, so the smears enter the twilight zone in other ways, such as by claiming that I lure people “to a page where he tries to sell you his anti-spam software.”
Ahem. I don't sell anti-spam software, and I never did. Several years ago, I developed a FREE site (MySpamSponge) that anyone can use to eliminate spam. I never charged for it, and I never will. I exploded this smear in more detail in an article in which I explained why I am very proud of the free service I created. The trusted intermediary concept I introduced to combating spam could be used in other ways (such as with snail mail) to make your life better, easier, and safer. In short, it's a great idea and something to be proud of, not ashamed of.
My opponents fear me because I write with intensity in a way that changes hearts and minds. However, those opponents are often so stupid that they can't even figure out where I stand on an issue, or they don't care to find out. In truth, when it comes to political matters, I don't favor the left or the right. I did in the past, but came to realize they're both far off base, seemingly trapped in a cycle of fighting each other because they haven't figured out what I did: a solution that could truly heal the nation and bring the left and right together by giving each almost everything they want. That seems impossible for inside-the-box thinkers, but it isn't (here's one example of how I could make even staunch Republicans and Democrats very happy). I am firmly convinced that our national economic problems can be overcome to the point that we have brighter futures than we ever imagined, but we cannot triumph by doing what we've been doing. We need good outside-the-box ideas, and we need to spend more time thinking than tearing one another down.
Speaking up is always risky. I could personally name the doughboy CEO mentioned above, but my informants that work at that hospital (all of whom think it's far from what a Top 100 hospital should be) fear they will be fired, so I'm waiting for them to leave in the near future.
A local doctor's wife thinks this supposedly Top 100 hospital is dangerous. Her young husband went there with a simple problem, but a medication overdose caused brain damage that ended his medical career (my informant said this doctor now has the intelligence of a young child). I heard she was paid to keep quiet and personally visited by a hospital big shot who expressed his deep sympathy. If they're so concerned about patients, why don't they do more to make that Top 100 nightmare a safer place?
One of my relatives went there with a dog bite, but they botched her care by making two major mistakes. They didn't even correctly utilize Steri-Strips! Calling that place a Top 100 hospital is like calling me an Olympic athlete after I broke my neck. Utterly absurd.
Now for the interesting part: I've worked in a hospital in which mistakes were so rare I never heard of any. Not one. The nurses and other staff knew what they were doing and everything flowed smoothly even when we were very busy. I credit the staff there but also the CEO, who was a genuinely friendly, down-to-earth person, not a detached snob like the Top 100 doughboy.
The right people make a huge difference.
Solving another mystery
Now to solve a perennial mystery: given that most hospitals have plenty of problems, why don't they solve the solvable ones? Even some of the ones with obvious solutions go unsolved for years or even decades, such as the aforementioned Top 100 hospital that permits its workers to wear uniforms outside the hospital, thereby helping spread dangerous and even deadly germs into the community. I worked in hospitals decades ago that provided uniforms they laundered, so I never went home in scrubs. Any hospital could launder uniforms, but the doughboy CEO's hospital doesn't do that, nor does it do many other things it could do to improve patient care and safeguard the community.
Why? The first reason is many people are threatened by change—even positive change. This especially pertains to people in charge. As bad as things may be now, they're at the top of the totem pole. The more things change, the greater the chance they'll no longer be on top.
The second reason is that the good ideas for change usually come from people not in command. If those ideas were acknowledged and implemented, it would validate their worth and hence the additional value of the innovator. Most big shots are more concerned with staying #1 than helping their corporation or hospital improve, so they often prefer to be #1 in a third-rate organization than #3 in a first-rate organization.
The third reason is that most people don't like creative ideas. They say they do, but researchers found that creative ideas elicited strongly negative reactions. They said that creative ideas “can trigger feelings of uncertainty that make most people uncomfortable.” Even when there is a desperate need for change and the creative solution is wholly positive, most folks prefer to cling to the old way of doing things.
I've seen this resistance to some of my political ideas. For example, I thought of a way to reduce welfare spending while giving more money to welfare recipients. That should thrill Republicans, Democrats, Libertarians, conservatives, liberals, the Tea Party folks, and everyone with a brain. It's a win-win-win situation:
- It's better for welfare recipients because they get more money—potentially much more.
- It's better for the government since there is less welfare burden to meet.
- It's better for taxpayers, who get to keep more of their money.
My plan would have many secondary benefits, such as helping reduce crime, improve education, and trigger the joy of helping others along with other priceless psychological benefits. It would make our society a better one, help people become better people, and warm hearts from sea to shining sea.
What's not to like about it? Well, it's different.
My principle could be applied to Social Security and various other government entitlement programs. Together, they are bankrupting our nation. We cannot solve our financial crisis simply by eliminating fraud and pork barrel spending such as funding research to see what college co-eds do in the dark after drinking beer—as if we didn't already know! We need to address entitlement spending, but politicians can only suggest reducing payments or restricting eligibility. That would help, but not enough unless the cutbacks were draconian. That way would generate much pain; my way is painless.
Thus, that one idea could help save the nation and determine if your children live in a nice home or hut, but people in power fear change, so they have their smear merchants attack, lie, distort, and twist words. They want to help themselves and their bosses keep the world the screwed-up place it is beset with myriad problems, and I want to help everyone solve our current problems and implement a more adaptive way of addressing problems in the future and, better yet, prevent them. It's all very doable, but the folks who oppose change would rather drag the world down and you with it.
My principle could also be applied to improving our national health. Let's say that you are a doctor, personal trainer, or anyone else with ways to help others lose weight easily. If you could help an overweight family go from thick to thin, you might be given a tax credit or other incentive. If you could help your entire community shape up, you'd be given a greater reward.
I've discovered ways to lose weight that are easy, painless, and sometimes even fun. When I got out of my residency program, I was so fat that I could not see my feet when I stood up. I was happy to be in a profession in which my white coat could camouflage a huge gut. I'd been given free food as a resident (one of the few perks doctors-in-training receive), and I took full advantage of it. Coupled with my virtually nonexistent willpower when it comes to food, I shoveled pecan pie into my mouth breakfast, lunch, and supper, along with two entrées and too much of everything. I rationalized this overeating by thinking of how I might be too busy to eat later, so I should stuff myself now, like a fat chipmunk getting ready for winter. Years of doing that made me look like a Pillsbury Doughboy™ who'd been inflated with an air compressor.
I wanted to lose weight once I began working as an attending ER doctor. I no longer had free food, but I had enough income to support my appetite in overdrive. I often ate an entire large pizza by myself, along with a pound of breadsticks oozing with grease. With my Mom not around to say no, one cookie became one box of cookies. I'd smother a plate full of hot dogs on buns with a pound of cheese and call it a snack.
I was fat and getting fatter, but then I discovered easy, painless ways to lose weight—perfect for someone like me with virtually no willpower. A year later, I was thin (29-inch waist) but regaining some of the strength that once enabled me to beat the captain of the high school football team and three others at the same time in an armwrestling contest. (I never exercised during medical school or residency.) The following picture, snapped by my Mom as I washed my new 1990 Plymouth Laser while visiting her on a weekend, attests to the success of my weight loss efforts:

People who think medicine must taste bad to be good are naturally skeptical of weight loss without willpower, but during that year I lost my blubber, not once did I starve myself or feel as if I were dieting. If it took willpower, I couldn't have done it, because I had none.
I've since learned many other ways to easily lose weight, so even though I am now much older and don't exercise after injuring a shoulder and breaking my neck, I am still in very good shape. I could teach my weight loss without willpower methods to the nation so we could all shape up. Since obesity contributes to so many diseases, that would save us countless billions of dollars and improve lives in priceless ways. If the government kept 99.99% of the savings and gave the rest to me, they would be happy, I would be happy, and Americans would be happier and healthier. Insurance companies could reduce their premiums, so healthcare would be more affordable. Thus, this would be another win-win-win situation.
A similar win-win-win situation could spring from disseminating the methods that enabled me to go from dunce to doctor. My sixth-grade teacher said I was “slow” (in front of the class, nonetheless!) and as late as the end of 10th grade, I had such difficulty in school that my plan to deal with it was to drop out and get a job in one of the Detroit auto manufacturing plants.
I mowed lawns and performed odd jobs over the summer as usual, but I also did something very unusual: I serendipitously stumbled upon a way to significantly boost brainpower: intelligence, memory, and creativity. When I returned to school in the fall, I could equal or surpass the performance of the school Einsteins. I got all A's and changed my career plans from working on an assembly line to medicine.
I went to college and did so well in it and on the MCAT exam that I was the one person accepted into my medical school class with just three years of college. My classmates congratulated me after I was accepted into Alpha Omega Alpha—the med school equivalent of Phi Beta Kappa—after my second med school year, which they said was a rare honor reserved for students with exceptional grades. I graduated in the top 1% of my class, the director of my residency program commented that I was the smartest resident they ever had, and one of my bosses said I was the smartest doctor he ever met.
Aren't these implausible accolades for someone who once was a class dunce? My boost in IQ and memory was significant but trivial compared with my creativity, which went into hyperdrive, flooding me with more ideas than I can develop. Properly managed, one of my best inventions could be the world's first multi-trillion-dollar idea. It's one of those things that seems impossible to do, but I successfully prototyped it and am in the fifth generation of its development, producing results that even I could not have imagined were possible just a year ago. Whomever buys the idea from me could make Bill Gates seem like a pauper and help the world be a much greater place. In solving one of the big problems, I developed a solution that also helps people in countless other ways. I'll save you lots of money, time, and improve your life in astounding ways. And that's just one of my ideas on how to make life better.
Some people who don't know what I am working on but just hear me vaguely referring to it claim I'm just full of hot air and enjoy bragging. My critics are, once again, dead wrong. (Skeptical? Read this.) I like to be an anonymous face in the crowd, not to stand out. When I worked in the ER, I preferred to work in hospitals far from where I lived. I had to be the center of attention in the ER—something my boss stressed to me—because I was the captain of the ship that patients and nurses looked to for guidance. After a 12- to 20-hour shift filled with more attention than any normal human wants, it was great to be anonymous, not Dr. Pezzi. When I shopped in areas I worked, even store clerks would comment on things I bought, such as by asking, “Is all that paper towel you're buying for the hospital?”
No, it's because I'm neurotically obsessed with cleanliness—or I was until I learned to let the housework slide so I could spend more time on inventions.
Americans love to idolize Hollywood stars, professional athletes, singers (especially when they're hot and dysfunctional), and gorgeous people. When those folks strut around like they're royalty, Americans lap it up and feed their egos. However, many American loathe anyone else who thinks they're better or just stand out in any way, even when they'd rather not stand out, such as me when I wanted to buy lots of paper towel without store clerks repeatedly making a big deal about it. If they noticed my paper towel, you think they'd notice when I purchased something to prevent pregnancy? Or a bottle of wine? Or both, which sent some minds reeling as to what I'd do that Saturday night?
Frankly, doctors get too much attention. I once said “hello” to a hospital employee on my way to lunch, and when I returned the hospital was buzzing with a rumor she began that I had the hots for her even though I wanted nothing more than to be as pleasant to her as I was to everyone else at work.
With 700,000 physicians in the United States and many other equally bright people in other occupations, the fact that I am a doctor isn't especially noteworthy. However, the fact that I once was such a dunce that one of my teachers couldn't help but disparage me in front of the class does make my accomplishments relevant to people who want more brainpower than what they have. By knowing where I began and where I ended up, whether in terms of weight loss or brainpower, people see evidence of my improvement.
In my mind, those marked transformations demonstrate that I have more potential to help others than people who figuratively were born on third base, yet act as if they just hit a triple. You know what I'm talking about: naturally slim, gorgeous women writing diet or beauty books, or people with high innate IQ tutoring others on how to improve their minds. Their self-help books are usually littered with basic tips everyone knows; if they were truthful, their primary tip would be: “Ensure you have the right parents; the right genes are so important!”
I can't help people unless they read my advice, which they likely won't do unless they understand this: while being a slim doctor isn't sufficient reason for others to pay attention, the fact that I once was a dunce and a blimp should make them see that I've come very far and could help them, too. Mentioning what I've accomplished is necessary for them to assess the end-point, so I do that, knowing that small-minded people who don't know what I am doing will accuse me of bragging. If that were my goal, I wouldn't waste my time. I once worried about my appearance when I was fat and covered with acne, but I later learned that almost no one cares about what others look like; they care about what they look like. Ditto for success and everything else. Hence, if I spoke of my accomplishments to brag, I could find much better ways to waste my time. No one cares about me; you care about you and your family.
One of the great joys in life is helping others, which is my motivation for speaking up, so I do.
A personal message to the doughboy →
In case you wondered about my enmity for many hospital administrators: They earned it by screwing patients, nurses, doctors, and other staff in unimaginable ways, creating situations in which mistakes were inevitable. I documented some of these in my books and ER websites (ERdoctor.com and ERbook.net). Not all administrators are bad; some are wonderful people, but too many are too ignorant of medicine to function well as medical executives while others are so unconcerned with patients that they must be sociopaths.
UPDATE: Some of the smartest and most powerful physicians at the Top 100 hospital discussed above didn't knuckle under to administration pressure to get the flu vaccine. They effectively told the hospital brass to buzz off, calling their bluff. The hospital threatened to suspend the staff privileges of noncompliant physicians. Will they follow through with their threat? Probably not. If they did, who would take care of their patients? The janitor? Docs in other specialties who don't know the first thing about the specialty of the docs who said no to the vaccine?
Related articles:
- Study suggests obesity may also impact flu transmission, not just severity of illness
Comment: Obesity increases the risk of severe complications from influenza, including death, and can increase viral shedding by 42 – 104%, thus spreading germs to more people. - Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community
Excerpt: “ … an association between repeated vaccination and increased viral aerosol generation … the association of current and prior year vaccination with increased shedding of influenza A …” - The uneasy, unbreakable link of money and medicine
- Doctors should question the value of most heavily promoted drugs: Findings suggest pharmaceutical promotion should be met with healthy scepticism
- Hospital bills are routinely inflated
- Medical Extortion, Fake Awards, and Assaulted by an ER Nurse
- Many physicians, clinicians work sick despite risk to patients, survey finds
Comment: Hospital employees are often pressured to work while they're sick, and sometimes threatened or fired if they don't. If hospital leaders truly cared about patients, they'd demand that workers with communicable infectious diseases stay home—but they don't. - “In 1910, Josephine Baker, M.D. started a program to teach hygiene to child care providers in New York. Thirty physicians sent a petition to the Mayor protesting that "it was ruining medical practice by ... keeping babies well."” Do doctors and hospitals truly want very healthy people? Do prostitutes want moralistic men with a healthy fear of disease?
- Nurses “risking the spread of superbugs by snubbing the in-house laundry service and washing their uniforms at home.” This article includes a photo of a nurse wearing a soiled uniform while standing next to vegetables in a grocery store.
- Vaccines Backfire: Veterinary Vaccines Found to Combine Into New Infectious Viruses based on Attenuated Vaccines Can Recombine to Form Virulent Field Viruses
- Poultry Disease Vaccine Brings Short-Term Results but Long-Term Problems based on The Effect of Vaccination on the Evolution and Population Dynamics of Avian Paramyxovirus-1
- Vaccines fail to protect obese mice from severe influenza infections
- Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren
- Are Flu Vaccines a Scam? (Excerpt: “Study after study shows the flu shot is a scam.”)
- Flu shot less effective for obese adults
- Flu vaccine same as last year’s: will you need to get it again?
- Boosting Body's Natural Flu Killers as Way to Offset Virus Mutation Problem
- Drug Companies & Doctors: A Story of Corruption by Dr. Marcia Angell, former editor of the New England Journal of Medicine and now a Senior Lecturer in the Department of Social Medicine at Harvard Medical School.
- The Truth About the Drug Companies: How They Deceive Us and What to Do About It by Marcia Angell, M.D.
- Is Academic Medicine for Sale? by Marcia Angell, M.D.
- More On Legal Remedies for Ghostwriting
- Ghostwriting Remains a Fundamental Problem in the Medical Literature
- Use Of Ghostwriters, Guest Authors Appears Frequent For Studies Involving Rofecoxib
- One in Five Medical Journal Articles Include Honorary and Ghost Authors, Study Finds
- Influence Of Drug Companies On Medical Literature
- Many Physicians Still Have Relationships With Industry, Survey Suggests
- Do Medical Schools Affect The Way Future Doctors Interact With Drug Companies?
- Impugning The Integrity Of Medical Science: The Adverse Effects Of Industry Influence
- Industry Sponsorship Leads to Bias in Reported Findings of Clinical Trials
- Side Effects Severely Under-Reported In ENT Medical Journals
- New Strategies To Tackle Medical Ghostwriting Are Debated
- Scientists unknowingly tweak experiments, article suggests
- News Media Often Do Not Report Potential Sources Of Bias In Medical Research
- Misleading Media Coverage Of Medicine
- Academics 'Guest Authoring' Ghostwritten Medical Journal Articles Should Be Charged With Fraud, Legal Experts Argue
- Study: Fraud growing in scientific research papers
- Misconduct, Not Error, Accounts for Most Scientific Paper Retractions: 10-Fold Increase in Fraud-Related Retractions Found
- Authorship Rules for Medical Journals Flouted by Pharma Industry, Experts Say
- Is It Possible Some Doctors Still Don’t “Get” the Extent of Big Pharma’s Financial Ties to “Standard of Care” Research?
- Dollars for Docs: How Industry Dollars Reach Your Doctors (search their database for health professionals or institutions who received drug company money)
- Eli Lilly and Company Physician Payment Registry
- Vaccine philosophical exemptions: A moral and ethical imperative by Alan Phillips, J.D.
- Most Will Be Mentally Ill at Some Point, Study Says (This New York Times article states that “More than half of Americans will develop a mental illness at some point in their lives.” This demonstrates the willingness of doctors to medicalize normal, common emotions so they can be treated with expensive drugs. Most folks can get over their troubles without medicine, especially if they know how nutrition impacts mood, thinking, and things that potentially affect mood, such as intelligence, creativity, and even sexual pleasure.)
- The Epidemic of Mental Illness: Why? by Marcia Angell, M.D.
- Special UV light safely kills airborne flu virus, finds study
- Inexpensive Infection Control Measures Could Save Thousands of Lives, Billions of Dollars (Excerpt: “At any given time, one of every 20 hospital patients has a hospital-acquired infection, [leading] to an estimated 99,000 deaths in the U.S. each year and up to $33 billion in preventable health care costs.”)
- Infecting Hospital Staff With Contagious Awareness (Excerpt: “Infections picked up in hospital affect almost a third of patients in intensive care, and kill 44% of those people.”)
- Hospital visitors also play a key role in infection control: Simple Hand-Washing Video For Visitors Could Reduce Rapidly Increasing Hospital Infection Rates
- Hospital Mobile Phones 'Superbug' Scare
- One in Six Mobile Phones in the UK Is Contaminated With Fecal Bacteria, Researchers Found
- Static Electric Fields as a Mediator of Hospital Infection
- Big Pharma Spends More On Advertising Than Research And Development (A big chunk of that marketing money is spent on wining and dining doctors as part of the drug rep T&A show.)
- Breakup of Physician, Drug Company Relationship Could Improve Health Care, Cut Cost
- Providing Free Drug Samples To Patients Risks Harm To Public Health, Experts Argue
- Doctors Not Informed of Harmful Effects of Medicines During Sales Visits
- Should Doctors Be 'Selling' Drugs For The Pharmaceutical Industry?
- Docs Not Immune to Drug Marketing, Study Finds
- Confessions of a Drug Rep
- Another day, another drug company cover up
- Follow the money: Medical reviews conclude influenza immunizations ineffective
- Swine flu advisers' ties to drug firms: Five WHO experts linked with vaccine producers
- Annual Flu Deaths: The Big Lie
- Following the Script: How Drug Reps Make Friends and Influence Doctors
- How To Win Doctors And Influence Prescriptions
- The Ethics of Selling Prescription Data
- How drug reps influence doctors: From free pens to elaborate three-course meals, Big Pharma is shameless about promoting itself. Sadly, it works.
- The Truth About Tamiflu: Has the U.S. wasted $1.5 billion on an ineffective drug?
- Children Who Get Flu Vaccine Have Three Times Risk Of Hospitalization For Flu, Study Suggests
- A medical researcher said, “Worrying about vitamin D toxicity is like worrying about drowning when you’re dying of thirst.”
- Brief Fever Common in Kids Given Influenza, Pneumococcal Vaccines Together
- Vaccines and Brain Inflammation
- Sleep Affects Potency of Vaccines based on Sleep and Antibody Response to Hepatitis B Vaccination
- Michigan Opposing Mandatory Vaccines
- Institute of Medicine adverse reactions report admits MMR vaccines cause measles, seizures, anaphylaxis and other health problems
- MRSA May Increase Mortality Rate by 50 Percent, Study Finds
- Methicillin-Resistant Staphylococcus aureus Colonization and Risk of Subsequent Infection in Critically Ill Children: Importance of Preventing Nosocomial Methicillin-Resistant Staphylococcus aureus Transmission (laymen link: Hospitalized Children Who Carry MRSA at Risk for Full-Blown Infections)
- Vitamin D and HIV: letting the sun shine in (Excerpt: “These findings help provide a biological explanation for the increased risk of more rapid disease progression observed in HIV-infected persons with low levels of vitamin D or with genetic variants within the vitamin D receptor that alter binding to vitamin D.”)
- Innate immune response and Th1 inflammation Vitamin D is key to activating the innate immune response that provides a crucial role in defending against infection.
- Shannon Brownlee and Jeanne Lenzer are the world's most gifted medical writers. Brownlee is the author of Overtreated: Why Too Much Medicine Is Making Us Sicker and Poorer.
- Industry Conflicts of Interest Are Pervasive Among Medical Guideline Panel Members, Experts Say (Excerpt: “Researchers ... found that conflicts of interest are prevalent and potentially underreported among individuals participating in the development of clinical practice guidelines, which inform standards of patient care.”)
- Cochrane Collaboration Urges Free Access to All Data from All Clinical Trials
- Experts Propose Restoring Invisible and Abandoned Trials 'to Correct the Scientific Record'
- Patients and Doctors Are Being Misled by Published Data On Medicines, Germany Study Suggests
- Half Of Trials Supporting FDA Applications Go Unpublished
- Publication Bias Found Among Trials Submitted To FDA: New Study
- Flaws in Popular Research Method Exposed
Comment: What passes for science is often highly unscientific. If I did something comparable in the days when I participated in online dating, I would have created a personal ad saying that 100% of women found me highly attractive, referring to the few who did, and ignoring the 99.9% who did not. By cherry-picking information, pharmaceutical companies can make their drugs seem more beneficial and less harmful than they really are. BTW, political partisans do the same thing by focusing on or magnifying the attributes of their candidates and ignoring or minimizing their drawbacks. - Unpublished Trial Data 'Violates an Ethical Obligation' to Study Participants, Say Researchers
- Low Reporting of Clinical Trial Data in Key U.S. Database, Study Shows
- Drug Trials Funded by Industry Are More Likely to Publish Favorable Results, Researchers Find
- Medicine's Secret Archives
- Selling Sickness: How the World's Biggest Pharmaceutical Companies Are Turning Us All Into Patients
- Our Daily Meds: How the Pharmaceutical Companies Transformed Themselves into Slick Marketing Machines and Hooked the Nation on Prescription Drugs
- Overdosed America : The Broken Promise of American Medicine
- White Coat, Black Hat: Adventures on the Dark Side of Medicine
- Death By Prescription: The Shocking Truth Behind an Overmedicated Nation
- The Emperor's New Drugs: Exploding the Antidepressant Myth
- Vaccine Epidemic: How Corporate Greed, Biased Science, and Coercive Government Threaten Our Human Rights, Our Health, and Our Children
- On the Take: How Medicine's Complicity with Big Business Can Endanger Your Health
- Medicine Cult - A Prescription for Side Effects and Death
- Doctors Are More Harmful Than Germs: How Surgery Can Be Hazardous to Your Health - And What to Do About It
- Deadly Spin: An Insurance Company Insider Speaks Out on How Corporate PR Is Killing Health Care and Deceiving Americans
- Side Effects: Death. Confessions of a Pharma-Insider
- The Whistleblower: Confessions of a Healthcare Hitman
- Confessions of an Rx Drug Pusher
- Obesity is associated with impaired immune response to influenza vaccination in humans
- New Material for Air Cleaner Filters That Captures Flu Viruses
- Personal clothing may spread respiratory infections within the NICU
- Why the flu vaccine is less effective in the elderly
- The Witch Hunt of Jenny McCarthy for Talking About Vaccines
- High drug price trend has 'infected' generics, experts say
- Hilarious, but true!
“The test of a first-rate intelligence is the ability to hold two opposed ideas in mind at the same time and still retain the ability to function.”
— F. Scott Fitzgerald
Reference: Imagining dialogue can boost critical thinking: Excerpt: “Examining an issue as a debate or dialogue between two sides helps people apply deeper, more sophisticated reasoning …”